
By James Cain
Globally, AIDS has been responsible for over 34 million deaths, orphaning tens of thousands of children over the years. In general, the situation is changing for the better. There are new, effective drugs and the life expectancy of the 36 million people currently living with HIV has risen considerably from what it was a decade ago. However, there are still challenges in the fight against HIV in regions which don’t adhere to most global trends, notably in the Middle East and North Africa region.
HIV positive people across the world have long had to fight for equal and fair access to government health services, but how much can actually be achieved when governments, particularly those in the Arab States, continue to refuse to even acknowledge the existence of HIV positive citizens, by not providing data about their situations?
According to a report released by the UN entitled “How AIDS changed everything”, the Middle East and North Africa region is one of only two regions in the world where the number of new HIV diagnoses is increasing year after year. The report, which was published in 2015, revealed that between the years 2000 and 2015, there were approximately 22,000 new diagnoses of HIV in the region. This figure represents a 26% rise in HIV cases over these five years.
Furthermore, despite the tremendous amount of work being done globally to reduce the number of AIDS-related deaths, particularly amongst key demographic target groups, we find that the MENA region is an outlier yet again. In 2014, official statistics revealed that around 12,000 people in MENA lost their lives as a result of having AIDS. With the number of AIDS-related deaths more than tripling between the years 2000 and 2014, it is reasonable to assume that there is some level of neglect for the issue in government circles, reflected in the absence of data.
Without accurate annual reporting, governments, health services and NGOs will be blind to any changes in circumstances, and thus unable to act appropriately.
If governments in the MENA region are failing to accurately report on death statistics, the question that follows, logically, is why? Why are government bodies failing to carry out the necessary surveys, reports and studies? The previously mentioned UN report examined also the level of HIV stigma within societies across the globe. The Middle East and North Africa region was consequently found to be the worst region in the world in terms of levels of stigma against HIV-positive people. For example, over 80% of respondents from the region answered “no” to the survey question: “Would you buy fresh vegetables from a shopkeeper with AIDS?”. It is therefore possible that this widespread stigma has filtered through from the opinions present in communities in countries like Jordan, and is now manifested in government’s apparent inability (or refusal) to accurately report on HIV-related issues. If this is the case, then government would be violating its duty to serve all of its citizens equally, and not to purposefully neglect and therefore endanger certain groups of citizens.
The groups of citizens most threatened by inaccurate reporting in this area are identified by the UN as: injecting drug users (IDU’s), men who have sex with men (MSM), and sex workers (male or female). These three groups are also the three UNAIDS target groups, which HIV campaigners urge governments worldwide to devote specific attention to in their efforts to combat AIDS. The inability of the Jordanian government to produce annual statistics examining the specific situation regarding HIV and AIDS in these three key demographic target groups represents a systematic problem which has been hereditary between successive government administrations and works to consistently discriminate against and endanger every citizen who falls into any one of these three categories.
How does Jordan compare to other countries in the MENA region?
According to the UNAIDS website, the data they release on HIV and AIDS prevalences and trends “is produced by countries and submitted to UNAIDS at the end of March every year.” It follows that should there be any gaps in the data, this is the fault of individual governments not producing annual reports.
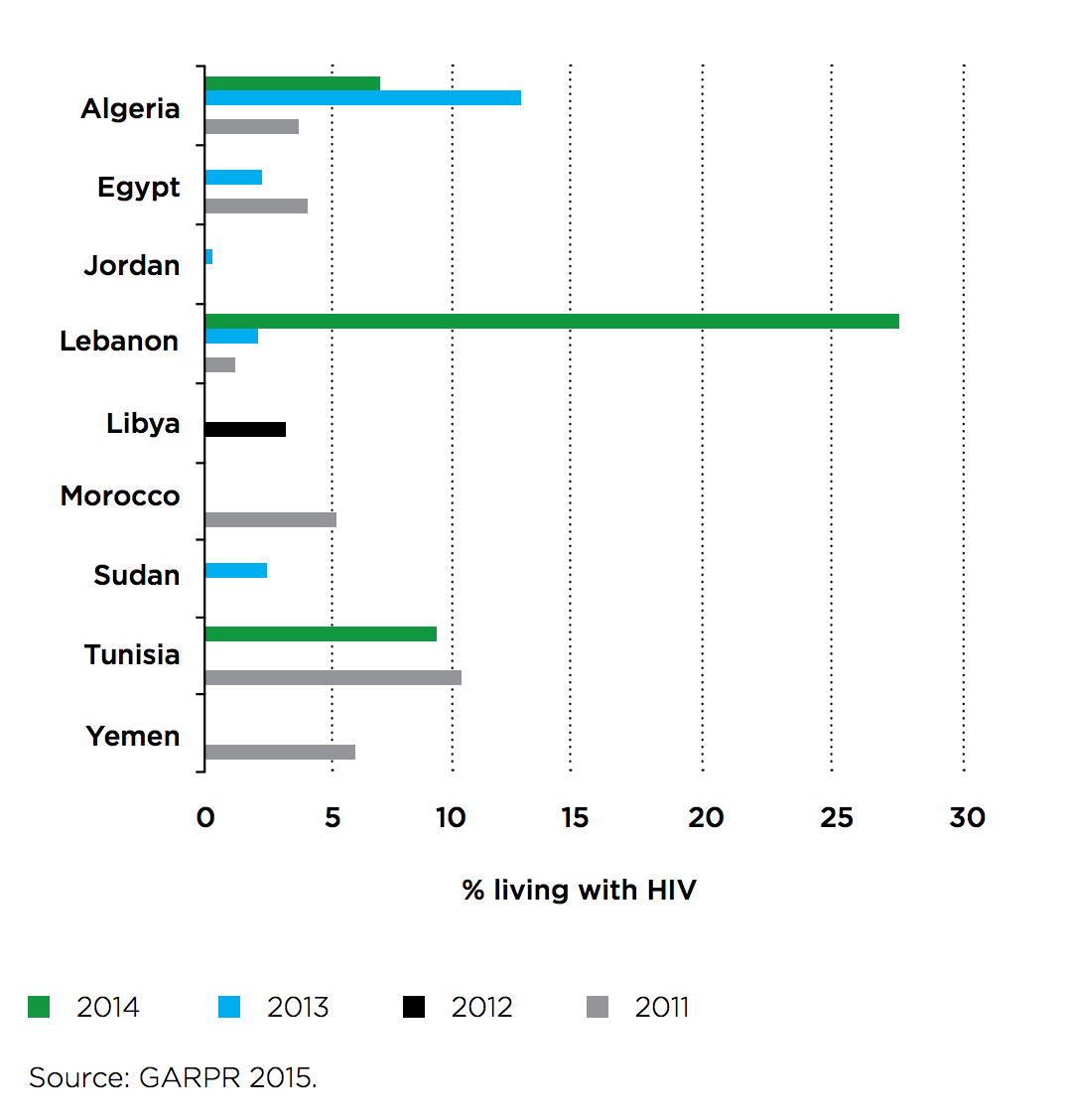
In the years 2011-2014, Algeria was one of the most consistent countries publishing data. The Algerian government cooperated with UNAIDS to produce four annual reports across the four years examining the situation within the female sex worker population, and furthermore three of the four annual reports also had a focus on MSM. Likewise Lebanon released annual figures examining HIV prevalences among MSM in the years, 2011, 2013 and 2014. Jordan however, released data just once in this four year period, in 2013.
This graph from the UNAIDS report displays all the data published in the MENA region, specifically about MSM and HIV. What it does demonstrate is that while some governments, such as the Algerian government, have a degree of consistency in reporting on this issue, the overwhelming majority of MENA governments do not publish data in any consistent manner. These nine countries are the only ones to have published any reports during that period.
Why is annual reporting so important?
It could be argued that the data released in 2013 by the Jordanian government is still useful. After all, it indicated very low levels of HIV in both MSM and female sex workers, so why should this issue be a priority for the government? To answer that question, we have to consider the data published by other countries in the region. For example, in 2013, Lebanon reported a HIV prevalence of 2.5% among MSM. In the same year Jordan reported a prevalence of under 1%. However the following year, in 2014, the Lebanese government released figures displaying a massive and apparently sudden increase in HIV prevalence in the MSM target group: over 27%. The point, which Lebanon proves perfectly, is that without accurate annual reporting, governments, health services and NGOs will be blind to any changes in circumstances, and thus unable to act appropriately. Consequently services for HIV patients will quickly become insufficient.
We spoke to Sharafdzon Boborakhimov, one of the international coordinators at Y-Peer, an NGO pioneered and funded by the UNFPA, which is very active in tackling issues such as HIV awareness in the Arab States. “In order to tackle HIV prevention and address youth and adolescent Sexual and Reproductive Health (SRH) issues, having correct and reliable governmental and non-governmental data is crucial,” he said. “For the Y-PEER network, having reliable data helps to develop and implement effective programs covering particular age groups of young people at risk and specific regions with highest rate of infection.”
What are the consequences of inaccurate reporting?
A lack of accurate reporting can endanger the lives of citizens in the MENA region. Arguably, this is already the case – AIDS related deaths have more than tripled in the region since 2000. More specifically though, governments which base their health policies on inaccurate or outdated statistics fail to contain the issue at hand, allowing it to spiral out of control.
Key areas in which the governments in the MENA region are failing include both providing effective anti-retroviral treatments to people diagnosed with HIV and providing HIV testing and STI screening to the population as a whole and specifically to the UNAIDS three target groups. When it comes to providing the necessary anti-retroviral treatments to HIV patients in MENA, UNAIDS estimates that only 14% of those who need such treatments are currently receiving them. Furthermore, HIV testing, according to UNAIDS, was not found to be common in the MENA region, with not a single country surpassing a testing-rate of 30%.
HIV, in this way, is as much a political disease as it is a viral disease.
The lack of accurate reporting affects this situation in two ways. First of all, due to the irregularity, infrequency and inaccuracy of available studies, governments underinvest in HIV prevention and treatment, meaning that such services, where available, are often grossly inadequate. Secondly, as a result of bad reporting, individual citizens have no way to gauge their own personal risk levels, meaning there is an increased likelihood for risk-taking behaviour, which in turn contributes to an increase in HIV rates. This is all then taking place in a society where there is intense stigmatisation of those at the highest risk of contracting HIV/AIDS. For example, there is an abundance of anecdotal evidence showing that many MSM in the MENA region are married to women, meaning their risk-taking behaviour then puts their wives at risk, without them knowing. If more studies were to be carried out on this issue, then more people would get tested and consequently more people would know their HIV status, thus lowering the general risk associated with sexual-sensation-seeking behaviours.
When trying to combat AIDS-related deaths, the most important thing is to encourage people to get tested for HIV. But in societies where stigma and shame are widespread there is much to deter at-risk individuals from being tested. The government therefore has the responsibility to challenge this stigma, in order to encourage those at-risk individuals to get tested. However this is not what we can see. Instead we see that governments foster stigma and succumb to ideas of shame, prioritising these over the health needs of individual citizens. HIV, in this way, is as much a political disease as it is a viral disease.
With the UNAIDS deadline for submitting country specific reports on HIV/AIDS having just passed us by, it will be interesting to see if the Jordanian government had carried out any studies this year, almost 4 years since the last figures were released.






